What EU Manufacturers Need to Know in 2026
If you build, launch, or maintain medical devices or IVDs in the EU, the MDR/IVDR targeted revision is the most consequential regulatory update since 2017. On 16 December 2025, the European Commission unveiled a proposal to simplify and streamline MDR and IVDR, cutting administrative drag while keeping safety standards intact.
From our side, 40+ consultants supporting manufacturers across the UK, US, Spain, Belgium, Portugal and the wider EU, we’ve already mapped the practical impact by role, class, and portfolio. Our team of experts analyzed the revision and wrote this article, with action steps you can start this quarter.
Download the complete regulatory analysis
Want the article-by-article breakdown, templates (structured NB dialogue, PSUR cadence, Basic UDI-DI timing), and role-based checklists?
The Big Picture: why the EU proposed a targeted revision
The Commission’s objective is simple: reduce burden, improve predictability, and protect innovation, without lowering safety or performance requirements. The move responds to structural bottlenecks (NB capacity, uneven practices, and certification timelines) that have strained SMEs and constrained product availability.
Team insight
In recent NB projects for UK and US manufacturers seeking EU CE, we’ve observed that early, structured NB engagement eliminates avoidable review loops and reduces time-to-decisionespecially for complex portfolios.
What actually changes (and what doesn’t)
The proposal retains MDR/IVDR safety foundations but changes how processes are applied, more proportionate and digital by default. Key areas:
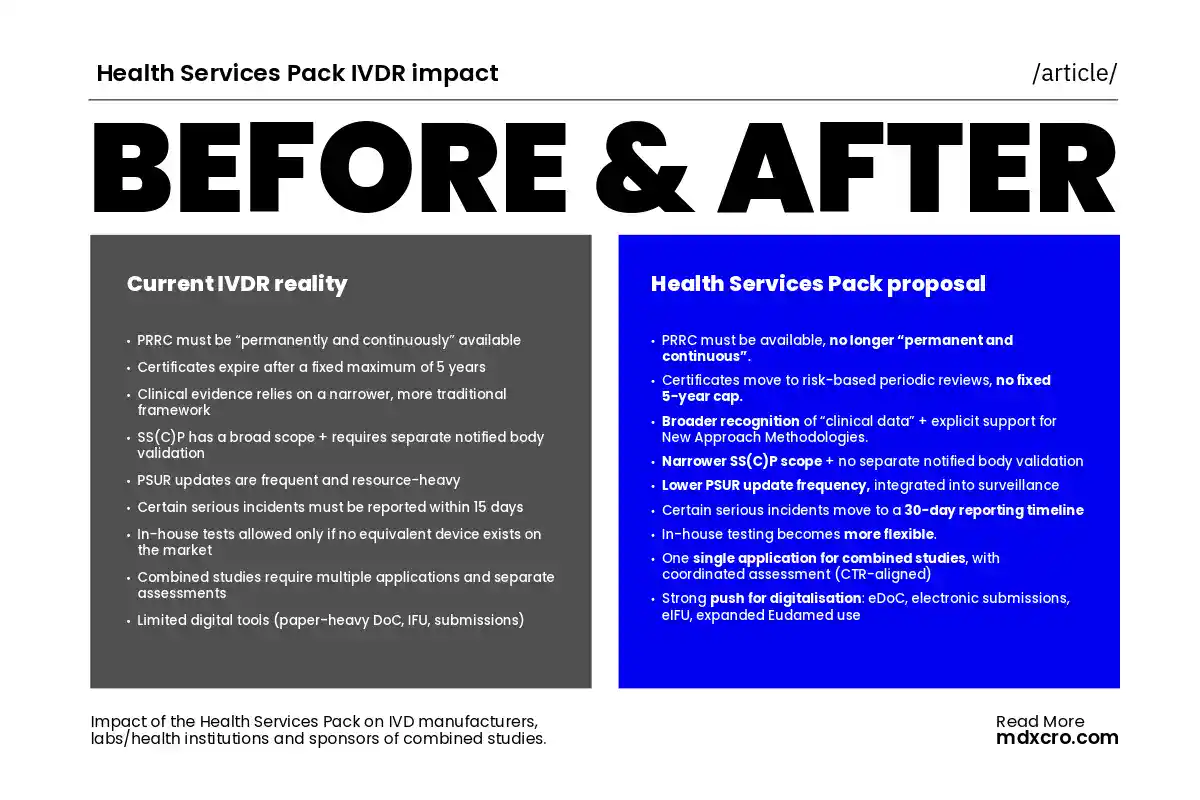
PRRC, certificate validity and risk-based reviews
- PRRC: Simplifies qualification requirements; SMEs using an external PRRC no longer need them “permanently and continuously” available—just available.
- Certificate validity: The fixed 5-year cycle is removed. Expect risk-based periodic reviews rather than hard recertification clocks.
Team insight
In multi-site recertifications, moving to risk-based reviews lets RA/QA concentrate on signals instead of calendar milestones, our clients expect a significant reduction in PSUR-related rework after sequencing updates with PMS findings.
PSUR & SSCP/SSP: lighter, risk-driven reporting
- PSUR: Class IIb/III (update in Year 1 and every 2 years after; Class IIa) only when necessary based on PMS. NB reviews PSURs for high-risk classes during surveillance.
- SSCP/SSP: Scope limited to devices under systematic TD assessment; no separate NB validation.
Classification tweaks: software, reusable instruments & more
Expect targeted rule adjustments that lower risk class for certain categories (e.g., some reusable surgical instruments, accessories to active implantables, software) with proportional evidence expectations-details to crystallise via the legislative process.
IVDR Focus: In-house Devices, Studies and Class C/D Impacts
- In-house devices (Article 5(5)): More flexibility, including the ability to transfer in-house devices where public health justifies it; removal of the “no equivalent on the market” condition; central labs for clinical trials fall under the in-house exemption.
- Performance studies: Routine blood draws no longer need prior authorisation; leftover-specimen companion diagnostic studies drop notification requirements.
Team insight
Early expert-panel advice for Class C/D IVDs has prevented costly re-works in multiple dossiers. The proposal formalises earlier, faster scientific input to use it.
Faster, Clearer Market Access
Structured dialogue with Notified Bodies (and change control plans)
The proposal creates a formal legal basis for structured dialogue pre and post-submission, plus pre-agreed change control plans to reduce surprises. It also distinguishes changes needing notification, approval, or none.
Breakthrough & orphan devices: priority and rolling reviews
New articles define breakthrough and orphan criteria with priority/rolling conformity assessment and expert access; legacy orphan devices may continue beyond transition under conditions.
Regulatory sandboxes for emerging tech
EU or MS-level sandboxes will enable supervised testing and data-generation for novel tech—accelerating de-risking while maintaining safeguards.
Team insight
For AI-enabled diagnostics, a sandbox + early panel advice creates a two-track plan (evidence + regulatory) that keeps development on schedule while aligning with cyber and data obligations.
Going Digital: EUDAMED, UDI and e-Labelling
The revision pushes digital-by-default:
- Digital DoC, electronic submissions, NB-manufacturer digital TD, and eIFU for near-patient tests.
- Online sales: essential ID and IFU must be available to users.
- UDI: Basic UDI-DI reinforced (assign before NB submission where applicable), more public UDI data, proportionality for small volumes/individualised devices, and preferential conditions for SMEs.
Separately, the Commission has signalled the EUDAMED clock and mandatory use in 2026, which amplifies the value of getting your UDI and EUDAMED data house in order now.
The MDR/IVDR targeted revision is a course correction: proportionate requirements, predictable reviews, and a digital backbone—without compromising safety. Manufacturers that act early—codifying structured NB engagement, recalibrating PSURs, and industrialising UDI/EUDAMED—will convert complexity into speed and resilience. Start with the 90-day plan; the rest gets easier.
Download the complete regulatory analysis
Want the article-by-article breakdown, templates (structured NB dialogue, PSUR cadence, Basic UDI-DI timing), and role-based checklists?
FAQ
No. The proposal keeps safety intact while simplifying process steps and aligning evidence with risk.
For IIb/III: update in Year 1 then every 2 years; IIa: update when necessary per PMS. NBs review PSURs for certain high-risk classes during surveillance.
A formal framework to engage NBs before/after submission, with change-control plans and clear differentiation of changes needing notification/approval/none.
More flexibility, including transfer options and inclusion of central labs for clinical trials within the exemption; removal of the “no equivalent device” clause.
Digital submissions, Basic UDI-DI before NB submission (where applicable), and broader public UDI data access; plan for 2026 EUDAMED milestones now.
Ready to transform regulatory complexity into competitive advantage?
Contact MDx today and let us support your journey through the next chapter of MDR and IVDR.